

I run marketing and data for NoCo Pest Solutions, which means I spend a lot of time watching numbers that most people never look at. Mosquito activity indexes. DSHS surveillance reports. Search trend data.
On May 20th, I was staring at a Google Trends chart for “West Nile virus” and the line had gone completely vertical.
For two months — March and April — it had flatlined in the mid-20s to low 30s. Normal baseline. Background noise. Then May 20th: 100. Peak interest. The highest point in the entire 90-day window. It dropped. Then it started climbing again. By June 5th it was back at 92.
I’ve been doing this long enough to know what that spike means. People don’t search for West Nile virus unless they have a reason to. A confirmed case in their county. A news alert. A neighbor who got sick. A dead crow in the backyard. That’s not curiosity. That’s proximity.
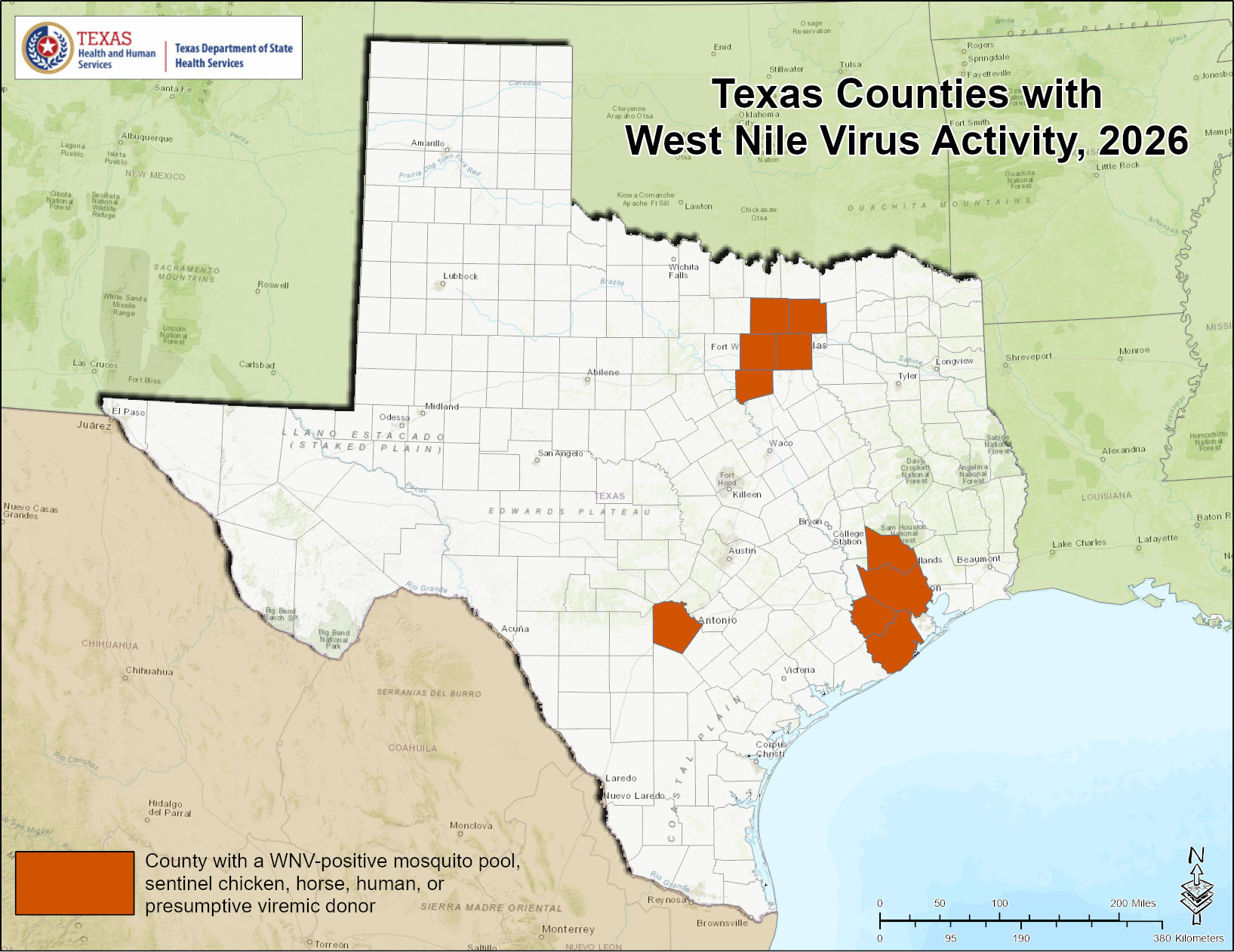
And if you live in Houston, Fort Worth, or Granbury — the Texas Department of State Health Services has already confirmed active WNV in your county this season. Harris County has averaged 35 human cases per year since 2002 — with 77 confirmed cases in 2024 alone. Local health officials describe the threat as “omnipresent.” The 2026 season’s first human case was neuroinvasive — the most dangerous classification — confirmed before Memorial Day.
I want to tell you exactly why that’s different than the same map showing up in Ohio or Oregon. Because the biology, the urban ecology, and the public health infrastructure in Texas create a fundamentally different threat profile. This isn’t me trying to sell you a mosquito service. This is what the research actually shows — and some of it genuinely surprised me when I dug into it.
Texas Is the National Epicenter. Not “One of the High-Risk States.” The Epicenter.
Let me put some numbers behind that claim, because this is the part that stopped me cold when I first pulled the full epidemiological record.
West Nile arrived in Texas in 2002. Between introduction and 2011 — nine full transmission seasons — the state recorded approximately 2,200 human cases. That’s a heavy endemic burden. Significant, but manageable. Then 2012 happened.
During the 2012 transmission season, Texas reported 1,868 human cases in a single year — nearly one-third of the entire national burden. Dallas County alone recorded 398 cases at an incidence rate of 16.0 per 100,000. Tarrant County — Fort Worth, our backyard — recorded 259 cases at 14.0 per 100,000. There were 89 confirmed deaths, a 5% case fatality rate. The aerial spraying campaign required to break the transmission cycle cost more than $47.6 million statewide.
That was a catastrophe by any metric. But here’s what keeps this relevant: Texas never stopped being a top-tier transmission state. In 2023, 54 human cases and 6 deaths. In 2024, 176 cases and 9 deaths by year-end. In 2025, with 115 cases reported by mid-season, Texas continues to rank at the top nationally alongside Colorado and Illinois — and that’s in the context of a year where severe neuroinvasive disease cases rose 41% and WNV deaths increased 32% compared to historical baselines.
This is not a once-a-decade event. It is a persistent, year-over-year threat embedded in the Texas environment.
I want you to sit with that 2025 number for a second: a 41% increase in severe neuroinvasive cases and a 32% increase in deaths compared to historical baselines — nationally — in a year that hasn’t finished yet. Texas is at the top of that list. Again.
It’s Not a Mutant Strain. It’s Your Backyard.
During the 2012 epidemic, the media ran with a narrative that a mutated, more virulent strain of West Nile was circulating in Texas. It was a compelling story. It was also wrong.
Researchers conducted complete genomic sequencing of 17 distinct WNV isolates from mosquito pools in Dallas and Montgomery Counties during the peak of the outbreak. What they found: two distinct genetic clades co-circulating, both genetically stable and functionally identical to strains from previous, milder seasons. No adaptive mutations. No amino acid changes associated with increased pathogenicity.
Dallas County had five times the human disease incidence of Montgomery County that year. The virus was the same in both counties.
Translation: The 2012 epidemic wasn’t caused by a scarier mosquito carrying a scarier pathogen. It was caused by a specific alignment of weather, ecology, and urban infrastructure that created the perfect amplification conditions. That combination can happen again. It’s happening in degrees right now.
The threat is your environment. Not an exotic mutation.
The Drought Paradox: When Dry Weather Means More Disease
Here’s the part that gets people wrong every time.
Conventional logic says rainfall creates mosquito breeding pools, so rain = more mosquitoes = more disease. In Texas, the dominant climatic variable correlated with WNV epidemics is the opposite: severe summer drought.
The “drought paradox” runs through several compounding mechanisms:
Ecological concentration. As regional wetlands and creeks dry up, birds and Culex mosquitoes are forced to congregate around remaining water — residential pools, irrigation systems, bayou remnants. High-density crowding dramatically increases vector-host contact rates, amplifying the virus through local bird populations at an accelerated pace.
Organic concentration in sewers. Drought eliminates the routine rainfall that flushes stormwater infrastructure. Without flushing, organic debris accumulates in catch basins and storm drains, creating concentrated, nutrient-rich water that accelerates Culex larval development — more mosquitoes, faster.
Desiccation-driven biting. Low humidity and high temperatures increase desiccation stress on female mosquitoes. To rehydrate and regulate water balance, they increase blood-feeding frequency. They bite you more. More bites = more transmission opportunities.
Immunosuppressed bird hosts. Heat and nutritional stress suppress the immune systems of avian reservoir species. Stressed birds develop higher, more prolonged viral loads. They become more efficient amplifying hosts, infecting a higher proportion of the mosquitoes that feed on them.
Meanwhile, warm winters set the stage. Longitudinal data from Dallas County shows a strong inverse relationship between the number of winter days below 28 degrees F and the scale of summer epidemics. Every mild winter preserves a larger population of infected adult female Culex mosquitoes in reproductive hibernation — ready to start the amplification cycle earlier in spring. Texas’s winters have been trending milder. Harris County Public Health officials told Axios this week that WNV activity started in mosquitoes in May 2025, persisted through the year, and trickled into 2026 — with migratory birds lingering longer into the season because of the warm winter as a contributing factor.
Put mild winter + dry spring together and you get 2012. You get 2024. You get the conditions that already produced Texas’s first neuroinvasive West Nile case of 2026 — in Harris County — before Memorial Day. Meanwhile, 49% of Texas was under active drought as of early June, with positive mosquito pools already confirmed in Tarrant County by DSHS. Both NoCo service areas are on the map right now.

The Houston Problem Is Not the Fort Worth Problem
The Southern House Mosquito (Culex quinquefasciatus) is the primary WNV vector in Texas — and she behaves differently depending on which city she lives in. Understanding the local ecology matters if you want to understand your actual risk.
Houston: It’s the Bayous. And Also Not the Bayous.
Harris County researchers analyzed 356 confirmed WNV cases and spatial controls across the county to map the precise relationship between the bayou system and human risk.
The counterintuitive finding: living close to the main bayou channels is actually protective, not dangerous. Proximity within 200 meters of major waterways reduced the odds of infection by a factor of 0.54. Why? Because Culex quinquefasciatus avoids open, flowing, predator-rich water. She wants stagnant, highly organic, sheltered pools. The main bayou channels — even the vegetated, slow-moving ones — aren’t her first choice.
What’s her first choice? The street ditches, residential storm drains, and standing water that forms in the residential neighborhoods away from the main channels. The water in the saucer under your potted plant. The clogged gutter you keep meaning to clear. The corner of the yard that never quite drains.
And at the suburban expansion corridors, there’s a separate driver: septic drainage systems. Aerated treatment units that discharge into open roadside ditches create a continuous supply of warm, organic-rich, nutrient-dense water. Culex larvae reared in sewage effluent develop faster, survive at higher rates, and produce larger adult females than those raised in clean rainwater. Suburban sprawl at the edges of Houston is essentially constructing custom Culex nurseries at scale.
Fort Worth: The Underground Threat
In the drier, more urbanized environment of North-Central Texas, the dominant driver is what’s under your street.
Thousands of miles of underground stormwater pipes, catch basins, and storm drains run beneath DFW. Due to structural settling, design limitations, and accumulated debris, these systems retain permanent pools of stagnant, organically enriched, thermally stable water — even during droughts. The concrete and soil insulate it from extreme heat. Predators can’t reach it. Female Culex enter through street grates to lay egg rafts, and the resulting adults emerge year-round.
There’s also a microclimatic accelerant specific to this area. The concrete mass of the urban core retains heat, keeping temperatures 2 degrees C to 4 degrees C warmer than surrounding rural zones. During summer, prevailing south-southeast winds carry this superheated air into the canopy-heavy residential neighborhoods to the north — areas like the Park Cities, Southlake, Keller. This warm air plume speeds both the mosquito development rate and the viral replication process inside the vector.
The storm sewer system breeds them at scale. The urban heat island accelerates the transmission cycle. And then the suburbs provide the ideal transmission environment.
That’s not theoretical. The Fort Worth Report confirmed in May 2026 that Tarrant County Public Health had already recorded positive WNV mosquito pools in Fort Worth and Grand Prairie — by May 14, out of 314 samples tested. The season was barely six weeks old.
The Park Cities Paradox: Why Wealth Isn’t Protection
Here’s the finding that stopped me completely when I first read it.
During the 2012 outbreak, epidemiologists documented a clear socioeconomic paradox: West Nile disproportionately hit affluent neighborhoods.
In the Park Cities — two of the wealthiest municipalities in Texas — WNV incidence rates were catastrophic. Highland Park recorded 34.3 per 100,000. University Park recorded 21.3 per 100,000. The City of Dallas as a whole recorded 7.8 per 100,000.
I had to read that twice. The wealthiest zip codes had incidence rates four to five times the city average. This isn’t a disease that tracks poverty the way most infectious diseases do. It tracks landscaping.
The mechanism is landscape, not behavior. Wealthy residential areas are defined by mature tree canopy, dense ornamental vegetation, and professionally maintained landscaping. During drought conditions — when everyone else’s yard dries out — these irrigated properties maintain moist soil, standing water in landscaping features, and a rich bird habitat. They concentrate every component of the transmission cycle: avian reservoir hosts nesting and foraging in the canopy, Culex vectors breeding in the irrigated irrigation runoff, and humans living and entertaining outdoors in the exact same space.
It’s not that wealthy neighborhoods are less aware or less cautious. It’s that the landscaping they’ve invested in is functionally an optimized WNV transmission environment.
If your neighborhood has mature trees, regular irrigation, and an active backyard — you’re in the high-risk profile. Full stop.
Who Gets Seriously Ill: The Real Risk Breakdown
The standard public health framing — “most people who get West Nile have no symptoms” — is technically true and functionally misleading.
Here’s the actual distribution:
- ~80% of infections produce no symptoms. No fever, no fatigue. They never know they had it.
- ~20% develop West Nile Fever — high fever, severe headache, body aches, fatigue, nausea, sometimes a rash. Most recover. It takes weeks.
- ~1 in 150 infected people develop West Nile Neuroinvasive Disease (WNND) — encephalitis, meningitis, or acute flaccid paralysis. These are serious. Some are fatal. Some survivors carry neurological effects for years.
In 2012, 844 of Texas’s 1,868 cases were classified as neuroinvasive — 45% of the total, with 89 deaths. That’s not a tail risk. That’s a 5% case fatality rate on confirmed cases, in a modern healthcare system, in the United States.
The demographic vulnerability data tells you specifically who faces the highest stakes:
- Age over 65: Odds ratio of 2.1 for developing neuroinvasive disease. The median age of WNV-related fatalities in Texas is 79 years.
- Male sex: 61% of neuroinvasive cases nationally, OR = 1.5.
- Essential hypertension (present in 37% of WNND cases), chronic kidney disease, multiple sclerosis (AHR = 2.34, the strongest single predictor of neurological progression), and hematologic malignancies all significantly increase severe outcome risk.
- Transplant recipients face a distinct threat: between 2002 and 2024, federal authorities documented 15 transplant-associated WNV transmission clusters in the United States. Most organ donors are not routinely screened for WNV. Houston and Dallas host some of the largest transplant programs in the country.
There is no vaccine. There is no antiviral treatment. Supportive care, and hope.
Translation: The 80% who feel nothing are statistically irrelevant to your personal decision-making. The 1-in-150 figure is an average across the entire infected population, including healthy 25-year-olds. If you’re over 60, have a chronic condition, or live with someone in either category, you are not the average.
The Governance Gap: Why $0.27 Per Person Isn’t Enough
Here’s the structural problem nobody wants to talk about — but I think you need to know, because it directly affects what level of protection you can realistically expect from your local government.
Vector control funding in Texas is fragmented, chronically underfunded, and wildly inconsistent across jurisdictions:
- Harris County (Houston): approximately $2.00 per person allocated to mosquito control.
- Tarrant County (Fort Worth): $0.27 to $0.30 per person.
- Hidalgo County (Rio Grande Valley): $0.05 per person.
For context, public willingness-to-pay surveys show that Texas residents would support paying an average of $53.15 annually in additional taxes for enhanced mosquito control and public health surveillance.
Tarrant County is spending $0.27 per person and residents say they’d willingly pay $53. That gap is not a rounding error. That is a public health system operating at roughly half a percent of the funding its own residents say they want to provide.
Texas is also a “Home Rule” state, meaning municipal governments retain substantial independent authority — including the authority to opt out of public health interventions. During the 2012 Dallas County emergency, when aerial adulticide spraying was identified as the necessary intervention to break the transmission cycle, each of the 44 municipalities within the county had to independently vote to authorize aircraft over their jurisdiction.
Thirteen of them voted no.
The result was a fragmented, patchwork treatment pattern with massive gaps. Researchers subsequently analyzed the difference in outcomes between aerially treated and untreated areas. Aerially treated areas achieved an incidence rate ratio of 26.42 post-treatment. Untreated areas: 10.57. Aerial spraying was 2.5 times more effective than ground-based treatment — and the communities that opted out got the inferior intervention during the deadliest part of the outbreak. The campaign is estimated to have prevented approximately 10 neuroinvasive cases, which translates to preventing 300 to 700 additional cases of West Nile fever.
The governance structure that allowed 13 municipalities to opt out of an aerial campaign during a public health emergency still exists today. The funding gap still exists. The fragmentation still exists.
I’m not saying this to be cynical about government. I’m saying it because understanding the gap is how you make a rational decision about your own property. Professional mosquito barrier treatment on your own property is the one intervention that doesn’t require your county’s budget cycle, your city council’s vote, or your neighbor’s agreement.
What “Professional-Grade” Actually Means Here
This context matters when we talk about what professional mosquito control actually does.
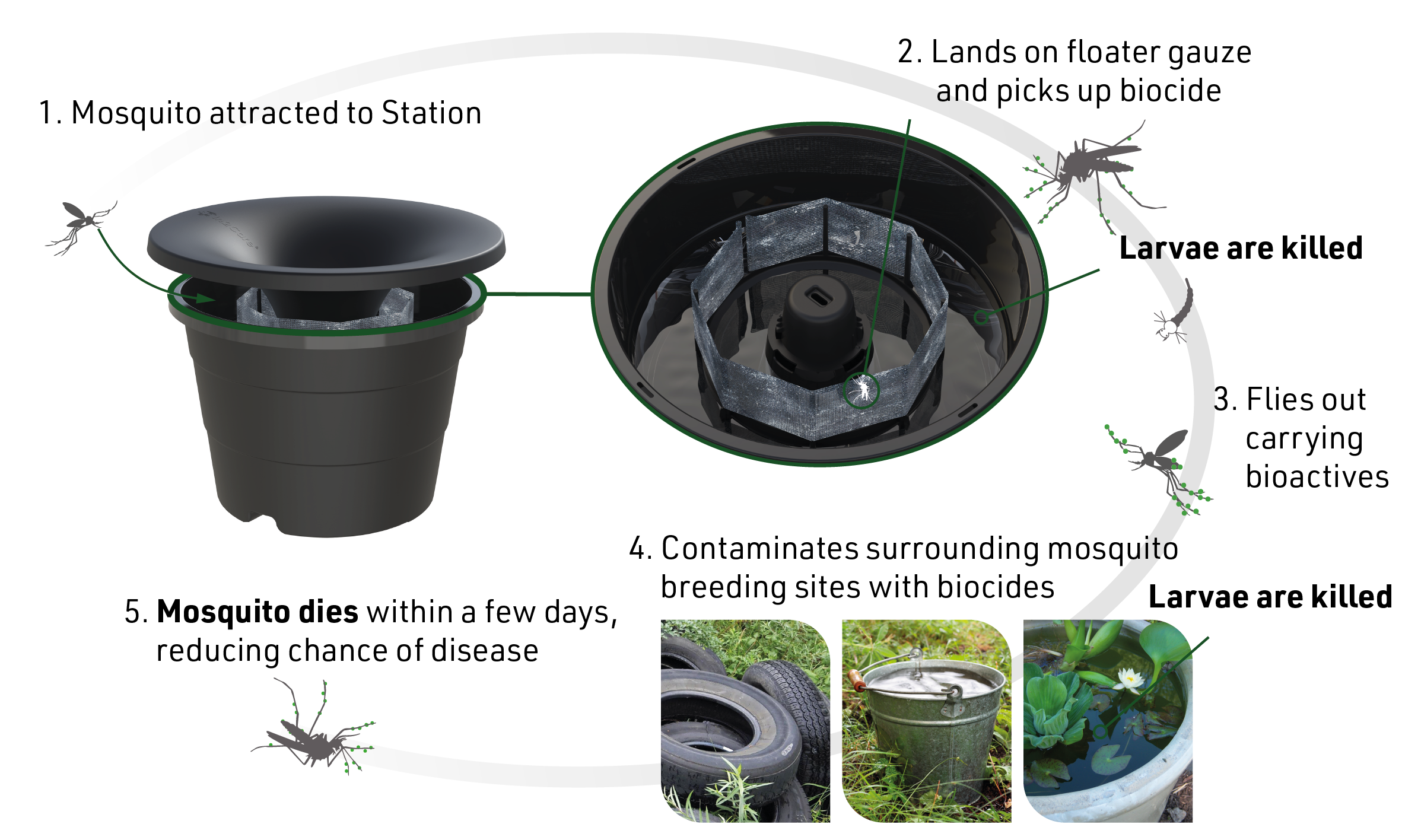
Products like the In2Care Mosquito Station are registered exclusively for licensed professional use — unavailable at retail, by design. The station lures egg-laying female Culex mosquitoes, loads them with a biological larvicide and slow-acting fungal bioactive, then releases them to contaminate every breeding site they visit before they die. It’s population control that reaches the subterranean storm drains and septic ditches that a spray rig never touches.
The barrier spray applied to your yard eliminates 85-95% of the adult mosquito population on your property. In the context of a county where $0.27 per person is what Tarrant County spends on vector control, your property isn’t waiting for a municipal cavalry that isn’t coming at full strength.
Monthly mosquito barrier treatment is a private-sector solution to a public infrastructure gap. That’s what it actually is right now in Texas.
The Timing Problem Nobody Talks About
Culex quinquefasciatus is a dusk-and-night biter. She’s not the mosquito that crashes your 3pm barbecue. She’s the one that bites you when you let the dog out at 9pm. When you sit on the patio after dinner. When you crack the bedroom window because the AC is running too cold.
The bites happen in the dark, in casual moments, with no drama attached to them. The incubation period for WNV in humans is 2 to 14 days. By the time any potential infection would develop, the connection to the mosquito is gone entirely.
This is why the Google Trends spike matters — and why the current June climb back toward the peak is the data point to watch. By the time people are searching at scale, the transmission cycle has been running for weeks. Confirmed human cases are a lagging indicator. The mosquito population carrying the virus is the leading one.
The treatment needs to come before the search spike, not because of it.
The Bottom Line
West Nile isn’t different for Texans because of bad luck or exotic biology. The research is unambiguous: it’s different because Texas’s mild winters preserve overwintering vector populations, summer droughts concentrate the transmission cycle, urban storm sewer systems provide year-round subterranean breeding infrastructure, affluent residential landscaping creates optimized transmission environments, and a decentralized governance structure ensures that public vector control is chronically underfunded and jurisdictionally fragmented.
The virus itself is genetically stable. It has been for 24 years. The environment it operates in is what makes it dangerous here.
2025 nationally is already 41% worse for neuroinvasive cases than historical baselines. Texas is in the top three states by burden. The DSHS 2026 map already shows confirmed activity in Tarrant and Harris and Fort Bend Counties. And the Google Trends data says people are actively searching for this right now.
The one lever you have direct control over is the mosquito population on your property.
Our monthly mosquito control service starts at $99 a month. No contracts. Cancel anytime. We’re scheduling Fort Worth and Houston treatments now.
The mosquito that gives you West Nile doesn’t announce itself. It bites you in the dark and moves on.
Get ahead of it.

